Diabetic Nephropathy (Diabetic kidney disease)
Diabetic nephropathy is a disease of the kidneys caused by diabetes.
What is the function of the kidneys?
Kidneys are bean-shaped organs located at the back of the body, at the bottom of the rib cage. Blood constantly flows through the kidneys where it is filtered and cleaned.
- The kidneys remove excess water and filter waste products from the body and pass them out in the urine.
- The kidneys also help to control blood pressure and produce hormones needed in producing red blood cells and keeping bones healthy.
If your blood pressure or blood glucose levels remain high over time, the risk of damage to your kidneys (diabetic nephropathy) can increase. The damage develops gradually over years, which is why it is called chronic kidney disease or CKD. It can range from a mild condition with no symptoms at all, to a very serious condition requiring dialysis or a kidney transplant. CKD is common but less than 1 in 10 people who develop the condition ever need dialysis or a transplant.
What happens in diabetic nephropathy?
In diabetic nephropathy, the filters of the kidneys, the glomeruli, become damaged. Because of this the kidneys ‘leak’ abnormal amounts of protein from the blood into the urine. The main protein that leaks out from the damaged kidneys is called albumin.
In normal healthy kidneys, only a tiny amount of albumin is found in the urine. A raised level of albumin in the urine is typically the first sign that the kidneys have become damaged by diabetes.
- Microalbuminuria is usually the first sign that diabetic kidney disease has developed and is defined as albumin in the urine between 30 and 300 mg per day. Over months or years, microalbuminuria may go away (especially if treated), persist at about the same level, or progress to proteinuria.
- Proteinuria is irreversible. Here, the amount of albumin that leaks into the urine is more than 300 mg per day. Persistent proteinuria usually marks the beginning of a gradual decline in kidney function.
How is diabetic nephropathy diagnosed and monitored?
In the diabetes clinic, you will be screened regularly to pick up the early stages of diabetic kidney disease.
- Blood test. This measures how well the body is filtering out waste products. The usual tests for this are
(1) estimated Glomerular Filtration Rate (eGFR) and
(2) creatinine level.
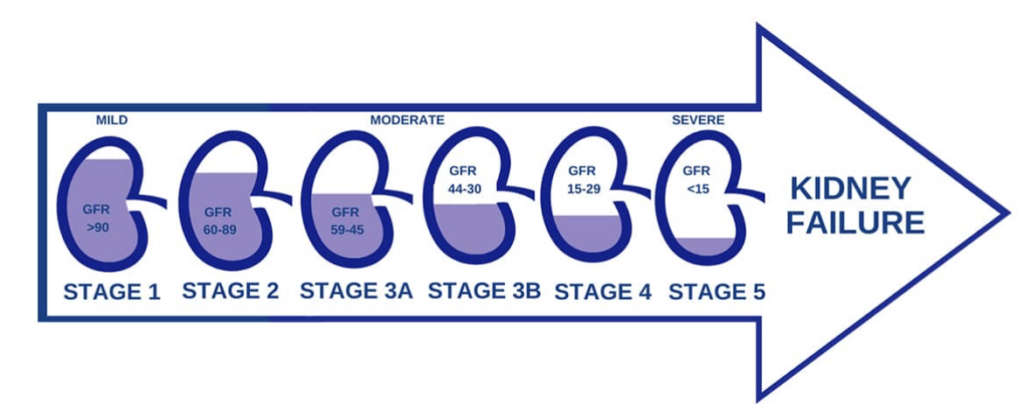
The estimated glomerular filtration rate (eGFR), is how much blood your kidneys can filter and clean every minute. This is more than 90 mL/minute in a young person with healthy kidneys. eGFR is used to grade the level of any CKD you may have. As the kidneys become more damaged, the amount of blood they are able to filter is reduced and the eGFR falls. Creatinine is a protein in the blood which is excreted in the urine. As CKD progresses and eGFR falls, blood creatinine rises.
- Urine test. An early morning sample of urine is best to measure microalbumin and protein.
If kidney damage is found, you will be given advice and treatment to protect the kidneys and prevent the damage from getting worse.
Stages of Chronic Kidney Disease
How is diabetic nephropathy treated?
Treatment aims to prevent or delay the progression of the disease. Also, it aims to reduce the risk of developing heart disease which is more common than average in people with diabetic nephropathy.
A slight increase in protein in your urine may be reversible by maintaining good blood glucose levels and normal blood pressure. Your doctor may also prescribe a type of medication called an ACE inhibitor or an Angiotensin Receptor Blocker (ARB) which can also slow down the process.
- Improving your diabetes control is the most important step to protect your kidneys. For example, if your HbA1c test result comes down from 9% to 7%, you will reduce your risk of kidney disease by 50%-70%. Agree on the right HbA1c target for you with your doctor, monitor your blood sugar levels and take your medication as advised. A newer group of diabetes medications called SGLT2I have also been shown to reduce the rate of progression of diabetic nephropathy.
- Achieving a healthy blood pressure. High blood pressure can make kidney damage worse, which in turn will increase your blood pressure. If your kidneys are already damaged it is important to maintain your blood pressure at normal levels. It may be helpful for you to monitor your own blood pressure so that you can act quickly on any changes. For most people, a target of 130/80 mmHg or less is recommended.
- Lose weight if you are overweight. Eat healthily and watch your salt intake. You may be asked to follow a low-protein diet.
- Keep your cholesterol level within a healthy range agreed with your doctor
- If you smoke, get help to stop.
- Taking prescribed medication, which usually includes angiotensin-converting enzyme (ACE) inhibitors or angiotensin-receptor blockers (ARBs).
- Avoid medications called non-steroidal anti-inflammatory drugs (NSAID’s) such as Ibuprofen and Diclofenac as these can worsen kidney damage.
- Attend your diabetes reviews.

What is the outlook?
- If you have microalbuminuria this may clear away, especially with treatment.
- If you have proteinuria over time the disease tends to become worse and progress to end-stage kidney failure. However, the length of time this takes can vary and it may take years.
- The main concern is the increased risk of developing cardiovascular disease. Cardiovascular diseases, such as heart attack and stroke, are the main causes of death in people with diabetic kidney disease. The treatments outlined above will reduce the risk of this occurring.
Dr Mohgah Elsheikh
MEMBER OF




